
Pelvic organ prolapse: when ‘saggy’ extends beyond your boobs.
This post may contain affiliate links. I receive a small commission through purchases made through these links at no cost to you. Thank you for supporting this blog!
It's possible that you clicked on this article wondering what else could possibly sag besides breasts, or you may be trying to put a name to a pelvic sensation you've had for a while. Or you may just be curious about pelvic organ prolapse, or POP. POP is a snappy name for the descent of the pelvic organs (bladder, uterus, colon, small intestine) due to stretch of these organs’ supporting ligaments or musculature. It is actually thought to be present at low grades in most women who have given birth (because stretch marks and a significant reduction in breast ‘perk' were not enough), although many women may not notice symptoms until menopause, or ever! By the time you get to menopause we can't really say what caused POP because so many things in life have happened since having kids (if it makes you feel better you can blame them, though). But you don't have to have carried or delivered a baby to develop a prolapse. This article will review the details of what POP is, risk factors, simple tools to avoid and/or manage it, and how to live the life you want with POP, because for any woman (but especially for younger women) a diagnosis can be devastating. If you make it to the end, I will provide some insight into my personal journey with POP.
As stated above, POP is the descent of pelvic organs. It may or may not be associated with any symptoms, but it is graded based on the level of descent from one to four, with grade one meaning minimal downward motion of the organ on assessment and grade four meaning the internal prolapsed tissue comes out of the body. In this article we will focus on vaginal and vaginal vault prolapses only-rectal prolapse does exist but will be outside the scope here. For terminology purposes, there are different kinds of prolapse: a cystocele is when the bladder descends into the front wall of the vagina; a rectocele is when the rectum descends into the back wall of the vagina; an enterocoele is when the small intestines descend into the back wall of the vagina; uterine prolapse occurs when the uterus descends into the vaginal vault (this can occur after hysterectomy, with descent of the vaginal vault irregardless of the presence of a cervix). The American College of Gynecology has videos demonstrating all of these pathologies, and I have created this very basic infographic below.
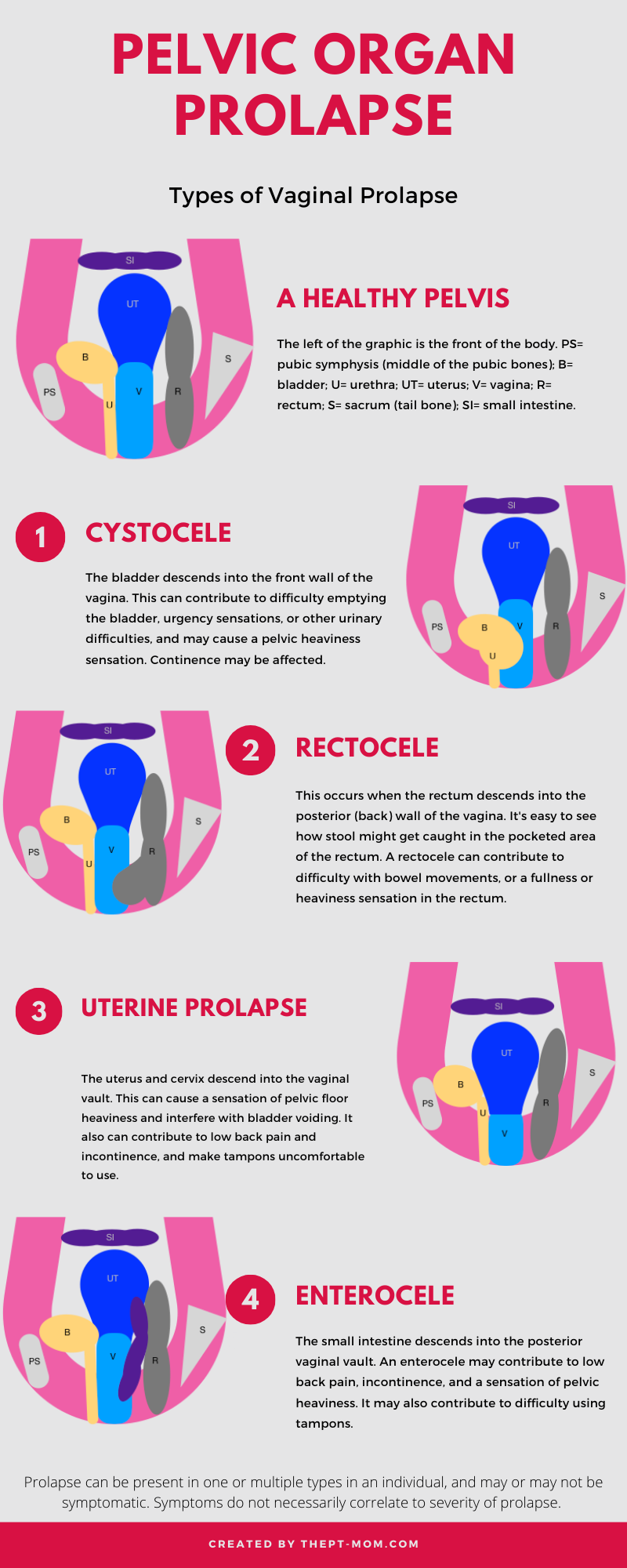
There are a number of ways the various organs can descend, and each woman will present differently in symptoms as well as have some anatomic variation in how the prolapse is situated in her body. There are multiple studies that show that some women with POP are asymptomatic. It has also been shown that up to 50% of women experience some level of POP after childbirth, indicating that this is a very common diagnosis. Women with the different forms of prolapse tend to display varying degrees of symptoms, but per the research the severity of symptoms do not necessarily correlate to the severity of the prolapse. Some reported symptoms for cystocele and uterine prolapse include urinary urgency, difficulty emptying the bladder completely, and stress incontinence, but reported symptoms vary more that those reported for posterior compartment (rectocele, enterocoele) POP. Women with a rectocele and/or cystocele prolapse display more consistent symptoms, which include difficulty emptying the bowels completely or the feeling of needing to strain to empty bowels. As you can see in the infographic above, the rectum will develop a little pocket and stool easily goes into this pocket instead of toward the anus. Women with a rectocele also commonly report needing to splint (place pressure on the perineum or pressure on the posterior vaginal wall) to completely void.
A huge percentage of women experience POP based on various studies, and as our population ages the numbers will increase. So if you are experiencing prolapse, take heart in that you are not alone in your journey and that medicine and science are continuing to advance greatly to improve outcomes for all of these pathologies (and hopefully work harder to prevent them). But why are so many women experiencing prolapse? There are many theories, some supported by the evidence and some I have that I think will be supported eventually.
Risk Factors
Below is a table from a study published in 2014 listing risk factors for pelvic organ prolapse:

As you read through this list don’t be alarmed, many of us can check off quite a few boxes here! But this list is actually pretty gray in terms of information instead of set-in-stone, black-and-white cause and effect. We really don’t have a specific recipe for who will or will not develop POP, or we would have practitioners saying who, specifically, should or should not have a vaginal birth, or who should stop at two kids. and which woman with a hysterectomy should be issued a pessary as prevention, etc. The bottom line is, all of these factors are interlinked and we don’t have some of these answers. As the paper linked above does point out, it is important to have a starting point to establish these risk factors, but there must be more studies so we can have a better foundation for prevention and management.
Some items in this table are well-established, clear risk factors. Connective tissue disorders specifically affect the same structures (ligaments, tendons, fascia) that help suspend our pelvic organs in their designated anatomical locations. Any of these disorders put you at higher risk for prolapse. And there are compounded factors not addressed here: age is listed, but not age at first birth which is a very important one. If tissue did not change with advancing age, the beauty industry would have no market. Just as your skin loses its youthful glow, your internal tissues are affected by age also. Your age during your first pregnancy/birth is a risk factor for levator ani avulsions, and the risk increases around age 30 and is significant at age 40. The levator ani are a deep muscle group that functions as part of your pelvic floor, and it can avulse, or tear, away from the bone (typically at the pubic symphysis-the front of the pelvis). This results in a varied intensity of compromised support for your pelvic organs depending on the severity of the avulsion. Having a large baby vaginally has also been linked (inconsistently) to levator avulsion. Age at all births following the first show much lower risk of avulsion.
This table also suggests that high impact exercise is a risk factor, however there have been multiple studies since its 2014 publication that have shown that high intensity exercise (CrossFit) does not show a significant difference in pelvic floor behavior versus low intensity exercise; and that the few studies that have looked at exercise and POP have found no correlation. Extremely strenuous exercise (paratrooper training-of course it’s been studied, though not common) is a risk factor for POP. Research has again left us in a gray area, with the extremely popular CrossFit workouts not showing negative effects, but it can be hard to know where to draw the line. So with this information, we can deduce that intense jumping on trampolines for long periods-or at the intensity professional trampolinists work in-may have a negative effect. And we know from another study that not all CrossFit exercises are created equal. Double unders cause a significant increase in intraabdominal pressure (more so than other typical CF exercises), which will ultimately exert pressure on the pelvic floor and organs. But double unders are not always regularly programmed at every gym, and when they are women may avoid them because of incontinence issues. So a woman who only does double unders versus the typical variety of CrossFit-type exercises may be more at risk. But again, it is truly a variety of risk factors that influence the outcome.
Avoiding/Minimizing Your Risk
While the risk factors may sound doom and gloomy, there are a number of factors that can be modified to prevent or reduce their risk of prolapse, or to minimize the risk of worsening a prolapse you already have. If you have the option of a operative vaginal or cesarean birth, consider the other risk factors and determine how high your risk for prolapse might be before deciding what is right for you. And both risk factors under bowel dysfunction are easily addressed (see my Pooping While Pregnant post, it’s relevant here even if you’re not pregnant). If you are chronically constipated and/or straining, that is very hard on your pelvic support system. Obesity, while harder to address, is excess weight placed on the pelvic floor and organs. If you can address it, you may notice a significant benefit if you have prolapse. If you have not developed prolapse, try to be proactive about your weight before menopause because at that point you lose some tissue integrity naturally and prolapse is a larger risk due to age and post-menopause status.
Another opportunity to address your risk factors is to address your intraabdominal pressure. This key term was hit on above, but it can be helpful to think of the core (abs to the front, diaphragm to the top, pelvic floor to the bottom, and spinal stabilizers to the back) as a juice box. If pressure is applied to one part of the ‘box’ or core, another part has to apply equal force to keep from giving way to the volume of juice. And if you have a weak area (think the straw hole was punctured), you always have an area that can’t control for the pressure changes. Very rarely is your diaphragm an issue, in part because of gravity, but if you don’t manage pressure well in your abs that may contribute to the development of a diastasis recti (separation of the abdominal wall between the six pack muscles). If you have a pelvic floor that can’t contract properly or provide a force equal to what is necessary to maintain integrity of your core, you may experience incontinence or prolapse. Back pain and weakness are symptoms of difficulty with your spinal stabilizers. All this is to say that the core needs to function in a way that allows for good pressure distribution. If you have an area of weakness, it is best to address it early on to avoid any development of tissue damage (diastasis, POP, etc) due to prolonged misuse. This is an excellent reason to go to physical therapy! Pelvic PTs are highly skilled at optimizing pressure mechanics!
Proper pooping also plays a role in minimizing risk. Scroll down for a how-to infographic!
What to do if you have prolapse
If you already have a prolapse (as stated above, it's not uncommon), there are so many things you can do to help ease your symptoms. First and foremost, address any endogenous issues. This means you must address chronic constipation, bladder habits, pelvic tension, intraabdominal pressure management, maintain a healthy weight, and learn your symptom triggers. There are others that I have not listed here, but starting with how your own body functions is key. You must also address these things regardless of if you plan to pursue corrective surgery or not, as they will give you the best outcome! Learning your symptom triggers is essential, although somewhat of a trial and error, to allowing yourself to find workarounds for tasks or activities that cause discomfort. If you still experience symptoms after addressing those issues, then consider other supporting tools. These other tools include pessaries (find a practitioner skilled in placement) during exercise only or full time (don’t worry, there are many variations so that if you are sexually active so you don’t have to ruin the mood to stop and take it out); use of supportive garments (see below); consider with your physician the use of topical estrogen for improved blood flow and tissue support; try various positions of hypopressives, which temporarily help to significantly reduce pressure on the pelvic floor; consider tools for splinting (also below) to help void bowel movements. AND MOST IMPORTANTLY, use excellent lubricant for sex. You want to enjoy that, not suffer in misery. Silicone-based lubricants provide the most reduction in friction, although there are water-based products that are also good.





For the images above:
The V2 supporter is great in pregnancy and beyond for reducing prolapse symptoms with gentle pelvic floor compression.
The Femmeze splint is very useful for improving the ease of bowel movements with a rectocele. It is easily washed between uses and is a discreet tool.
The Revive Activity splint is useful for determining if you might benefit from a pessary during activity (ie: running or weight training) to control POP symptoms-one of which may be leakage, however it might also help to control for feeling extra organ movement or soreness. *I don’t recommend it as a sole solution for reducing activity-related incontinence as there are multiple reasons that could contribute, and it should be further investigated prior to self-treating. There is also another brand that performs the same function (Poise Impressa).
VMagic is an excellent alternative for those not wishing to consider topical estrogen for various reasons. It is a natural vulvar moisturizer that can be used as massage cream. Daily massage has been shown to improve blood flow to the vulvar tissues, and will thus contribute to helping support the pelvic floor and organs.
There are a number of silicone lubricants on the market. I like this one, but look for one with minimal ingredients. If you want something more natural but still more helpful than water-based products, try plain coconut oil!
How to manage your symptoms with prolapse is very much in the pelvic physical therapy realm of expertise. If you don’t have a therapist you are working with, you should get one that you trust. A person who can help you systematically track your triggers and help you develop workarounds is essential. And he or she can also really help to guide your intraabdominal pressure management on return to higher intensity exercise if that is your goal (I have a post on this here, but it is best especially for prolapse to work through pressure management with a professional). Working with an experienced professional will help you to see the best results the fastest. And hopefully to get you back to doing whatever you want! Prolapse is not the end of your body’s function, and there are so many components to address to see where you can best make the most positive change. I also mentioned above that maintaining a healthy weight is important, and this is related to the amount of weight your pelvic floor and organs are supporting. It may seem really challenging to maintain weight while dealing with prolapse symptoms, and a physical therapist or skilled personal trainer can help you navigate different activities that will help you remain active without aggravating the prolapse.
My POP Journey

I developed a prolapse after the birth of my first child, probably related to his somewhat dramatic entry into the world because I had no issues throughout pregnancy. After his head was birthed, the cord was wrapped around his neck and the midwife reached to it off. At that point the cord broke and that took his already frustrating birth to an emergency level. My midwife basically reached in a grabbed him out as one would for a baby with shoulder dystocia (think full hand, wrist, and baby in what was once a small opening). Obviously, I would much rather have prolapse than risk my son’s life. And even though I am so grateful for how things turned out, it took me a long time to be ok with my ‘new’ physical normal. It also took me a long time to realize that my healing was way more delayed than it should have been, and that prolapse was one of the reasons for that. I sat on ice for weeks, and was so uncomfortable baby wearing (and still am to this day).
In the years since my son’s birth, I have come to peace with all the things that contributed to my prolapse (my placenta was also manually retrieved, I think I was starting to hemorrhage so hopefully that was essential!), but I read and did everything I could find on improving birth outcomes for my second child. And my second experience was much better, with much faster healing (although this is normal for a second birth; after you birth one watermelon, the second is easier). As I mentioned, I still get discomfort with baby wearing on the front and sometimes with a kid hiking pack on. But we do it anyway because my kids love it. My personal philosophy is that I’m not too concerned if my symptoms flare up, because we really don’t know if that actually equates to advancing prolapse. And I’m not going to miss out on things I want to do because my pelvic floor might be sad the next day! That’s not to say that I have not worked my way through my own advice here, that has been an essential part of my own journey and one of the reasons I stand firmly behind everything I suggest here. As you may know if you have read any of my fitness posts, I really enjoy working out. I feel that staying strong in my body carries over to strength in my pelvic floor, which is protective for POP!
I hope you have gotten some helpful information from this article. If you have any questions, feel free to comment here or find me on Instagram @thept_mom or Facebook as The PT-Mom! I will hopefully publish something soon on how to optimize birth to avoid or minimize your risk for POP!
Got Constipation? See this chart!!
